Neutropenia
in General Practice
By Associate Professor Chris Barnes
Published December 2021
Neutropenia is a common laboratory abnormality which may be detected incidentally during routine investigations. Reference ranges for neutrophil counts vary with age and ethnicity. A neutrophil count less than 1.5 X 10^9/l is considered low with severe neutropenia defined as a neutrophil count less than 0.5 X 10^9/l. Neutrophils are essential components of the immune system and neutropenia may be associated with a risk of life threatening infections, with this risk increasing with the degree of neutropenia.
Benign ethnic neutropenia
Benign ethnic neutropenia (BEN) is a condition observed in individuals of African descent and is characterised by a reduced absolute neutrophil count of less than 1.50 X 10^9/l in the absence of secondary causes. In contrast to other causes of neutropenia, BEN does not increase risk of oral or systemic infections.
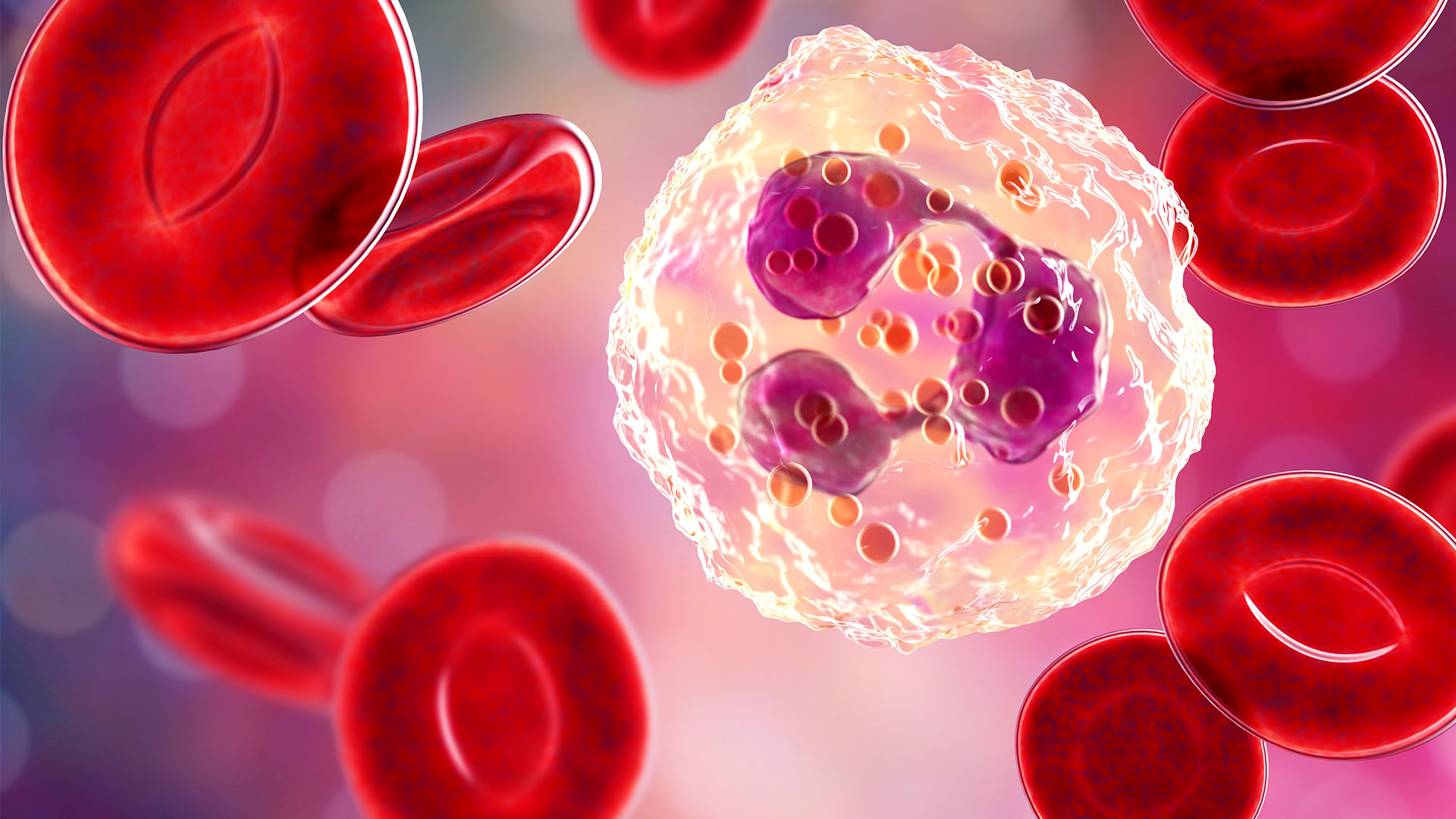
Function of the neutrophil
Neutrophils are produced in the bone marrow in very large numbers (approximately 100 billion are produced each day). Neutrophils monitor for microbial infection and respond with phagocytosis, degranulation and the formation of neutrophil extracellular traps (NETS) responsible for containing microbial infection that is too large to be ingested. Neutrophils are also a critical part of the immune and inflammatory pathways responding by producing cytokines and other inflammatory factors (Rosales Front Physiol 2018).
Causes of neutropenia
Mild neutropenia
Mild neutropenia (a neutrophil count ranging
from 1.0 – 1.5 X 10^9/l) is a common laboratory abnormality. Usually not associated with any
impairment of host defence, the cause for the mild abnormality does warrant further investigation.
Common causes for transient neutropenia include viral infections such as Epstein-Barr virus infection.
In children, chronic (> 3 months) mild neutropenia may be secondary to chronic autoimmune
neutropenia of childhood which resolves spontaneously by 3–5 years of age and may last for a median of
17 months. Chronic mild neutropenia in adults may also be secondary to mild autoimmune disorders.
Patients with mild autoimmune neutropenia generally do not have an increased incidence of infection
and may respond to infection with an increase in the neutrophil count. It is worth considering
neutropenia as a sign of a broader autoimmune disorder in patients who present with symptoms of
arthralgia, joint stiffness or rashes.
Medications including anticonvulsants, antipsychotics and chemotherapy are all recognised to be associated with neutropenia.
Nutritional neutropenia
Nutritional neutropenia may be secondary to
deficiencies of vitamin B12 and folic acid or copper or may occur in the setting of severe
malnutrition. Typically, nutritional causes are associated with additional cytopenias.
Persistent severe neutropenia
Persistent severe neutropenia (neutrophil count
less than 0.5 X 10^9/l) may be associated with a significantly increased risk of overwhelming
infection. Causes for severe neutropenia include severe congenital neutropenia. Whilst severe
neutropenia in older patients may be secondary to medication effects or even occur as a result of
autoimmune or post-viral conditions, bone marrow failure syndromes should be considered. In elderly
patients, severe neutropenia may be a manifestation of a myelodysplastic syndrome or bone marrow
infiltration disorder.
Work up of a patient with neutropenia
Careful history taking and examination is critical in the assessment of patients presenting with neutropenia. An understanding of the patient’s ethnicity including any family history is also important. It is helpful to enquire regarding illnesses around the onset of neutropenia and the presence of any symptoms of mucosal inflammation. A history of infections requiring their treatment with antibiotics or surgical drainage is important to know in order to understand the clinical significance of the neutropenia. A thorough physical examination including assessment for stigmata of autoimmune disease and presence of organomegaly is important.
The full blood count is central in the evaluation of patients presenting with neutropenia. The presence of additional cytopenias raises the possibility of a bone marrow failure syndrome. It may be appropriate to assess the neutrophil count on a repeated basis over 3 months to determine if the neutropenia is persistent. Correlation with any past full blood count analysis can be very helpful. In the setting of clinical suspicion of autoimmune disease, assessment of auto antibodies including ANA may be helpful. If an immunodeficiency is being considered, assessment of immunoglobulin levels is recommended. Assessment of haematinics may be important in the setting of concern about nutritional deficiencies.
Anti-neutrophil antibody testing is generally not recommended, acknowledging that the findings may be affected by high false-positive and false-negative results. Anti-neutrophil antibody testing is generally only performed by specialist reference laboratories.
A bone marrow examination can be helpful in patients presenting with neutropenia associated with other full blood count abnormalities or in patients presenting with unexplained chronic marked neutropenia. Bone marrow examination can be helpful to exclude myelodysplastic syndromes in elderly patients. Next generation sequencing is emerging as a useful tool particularly in the assessment of young patients presenting with severe neutropenia.
If you enjoyed this article, subscribe to our electronic Pathology Focus newsletter.
Subscribe Today!
About the Author

Associate Professor Chris Barnes
MBBS FRACP FRCPAAssociate Professor Chris Barnes
MBBS FRACP FRCPA- non–malignant haematological conditions including…
- paediatric haematology
Associate Professor Chris Barnes joined Clinical Labs in 2016 and is the National Director of Clinical Pathology. Prior to this, he worked as a consultant haematopathologist with Healthscope Pathology from 2009. Chris is a dual-trained clinical and laboratory haematologist, having trained at the Royal Children’s Hospital and the Royal Melbourne Hospital. He also undertook training at The Hospital for Sick Children in Toronto, Canada. He holds a part-time public hospital appointment at the Royal Children’s Hospital, where he serves as the Director of the Henry Ekert Haemophilia Treatment Centre. Chris has extensive clinical research interests and is the principal investigator on eight separate clinical trials based at the Murdoch Children’s Research Institute. He has held numerous leadership positions, including Chair of the Medical Staff Association at the Royal Children’s Hospital and Chair of the Australian Haemophilia Directors Association. He is currently the Chair of the Australian Bleeding Disorders Registry with the National Blood Authority and a Director of Melbourne Haematology and Melbourne Paediatric Specialists. Chris’ focus within Clinical Labs is the national supervision and management of clinical pathology disciplines, including haematology, biochemistry, microbiology and immunopathology.
Local Pathologists
 Pathologist
Pathologist
 Pathologist
Pathologist
Related Pages
Iron Deficiency in Women
Associate Professor Chris Barnes discusses the prevalence of iron deficiency in women, its symptoms, diagnostic strategies and effective treatment options.
Iron Infusions and Hypophosphatemia
Associate Professor Chris Barnes discusses the prevalence of iron deficiency anaemia, treatment options including iron infusions and managing hypophosphatemia risk.
Investigating Fatigue in Women
Associate Professor Chris Barnes explores modern approaches to diagnosing fatigue in women, offering clinical recommendations to improve patient outcomes.